What is a sarcoma?
As we briefly touched on in What are the types of uterine cancer, the uterus can give rise to different kinds of tumors. Those that develop out of the muscle or supporting tissue of the uterus are called sarcomas. These are very different from the endometrial cancers discussed earlier, both in their behavior and their prognosis.
Sarcoma: Tumor that develops out of the muscle or supporting tissue ofthe uterus.

Are there different types ofuterine sarcoma?
There are three main types of sarcomas of the uterus. Those that arise from the muscle are called leiomyosarcomas and account for about 30% of all sarcomas of the uterus. They can occur at any age but the majority occur in women in their fifties. A more common type typically seen in postmenopausal women, and that accounts for up to 50% of these cancers, are carcinosarcomas.
These are dual cancers with an epithelial component(carcino-) and the sarcoma component. They can also arise in the ovary and other sites in the female tract but are commonly seen in the uterus. In carcinosarcomas, the muscular-cancer can appear as tissue that is native to the uterus (called homologous) or interestingly, it can grow as tissue that is not normally found in the uterus, such as bone or cartilage (called heterologous).
Finally, there are endometrial stromal sarcomas, which do not arise from the muscle, but from the supporting tissue of the uterus (called the stroma).These account for about 15% of tumors and typically are responsive to estrogen. There are other rare sarcomas, such as adenosarcomas, which unlike carcinosarcomas have a nonmalignant epithelial component (the “adeno-”part), and rhabdomyosarcomas, but the most common ones are those previously listed.
Carcinosarcomas: Dual cancers with an epithelial component(carcino-) and the sarcoma component.
Endometrial stromal sarcomas: Cancers which do not arise from the muscle, but from the supporting tissue of the uterus (called the stroma).
Stroma: Supporting tissue of the uterus.
Are there risk factors for uterine sarcomas?
The only established risk factor is prior pelvic radiation, which is associated with 10% to 25% of these types of cancers. There is a very small risk of uterine sarcomas, particularly for carcinosarcomas, in women who take Tamoxifen. Otherwise, there are no other known risk factors for this.
Are there symptoms for uterine sarcomas?
There are no specific symptoms for uterine sarcomas. The signs of a potential uterine cancer apply to these tumors as well. Thus, any evidence of abnormal bleeding (i.e.,not part of a normal menses, postmenopausal bleeding, or particularly heavy bleeding),a sensation of abdominal pain or fullness, increased frequency of urination, or a mass in the vagina, are all signs of uterine cancer, and may be seen with uterine sarcomas.
What kind of surgery is done for uterine sarcomas?
Both the diagnosis and staging of uterine sarcomas have been adapted by the approach to endometrial cancers. Surgery is still the mainstay of treatment and the approach is determined by how large and/or how advanced the cancer is at diagnosis. The lymph nodes are at risk for being involved with carcinosarcomas, so a node dissection is performed. However, a study from Memorial Sloan-Kettering Cancer Center suggests that if leiomyosarcomas are isolated to the uterus or pelvis, then the lymph nodes are not usually involved. Given this, women who have leiomyosarcomas should have nodes removed only if their surgeon feels they look suspicious. For any woman with uterine cancer, though, a careful inspection of the entire abdomen and pelvis is required. Surgery is best performed by a Gynecologic Oncologist.
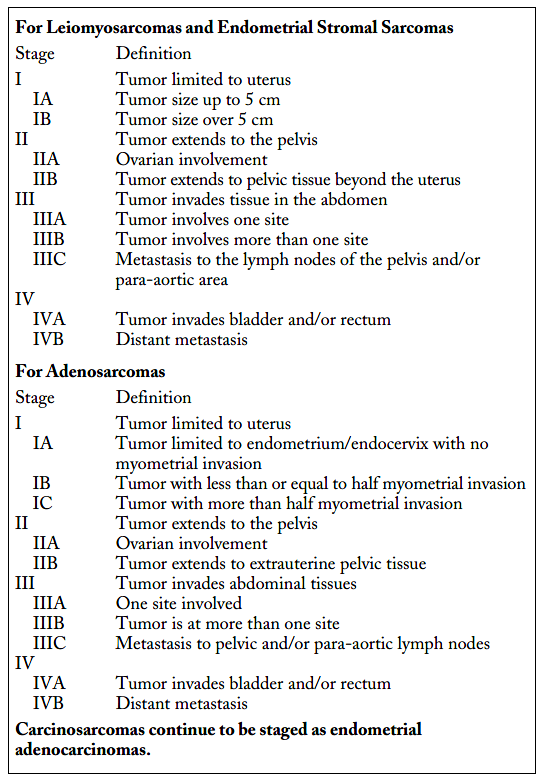
The staging of uterine sarcomas has been separated from that of endometrial cancers in the most recent FIGO classification system. It is as follows:
What kind of treatment is given for sarcomas?
We have no evidence that treatment after surgery is of benefit for women with uterine sarcomas, and this applies to both the use of chemotherapy and to the use of radiation therapy. However, treatment with chemotherapy or radiation (or both) is highly individualized to the patient and her physician’s preference.
Radiation can be directed to the pelvis only or may be given to the entire abdomen, and much depends on what type of sarcoma you have and how extensive it was when found.
Women with carcinosarcomas were studied in a large randomized trial where half received whole abdominal radiation and the other half a combination chemotherapy regimen using the drugs ifosfamide and cisplatin. This study showed that chemotherapy reduced the risk of recurrence by 30% and also improved survival over radiation alone. This suggests that chemotherapy may play a large role in treating these specific sarcomas.
What is my prognosis?
Uterine sarcomas are generally very aggressive, though the risk of having it return is most closely linked to grade and stage. That is, grade 3 sarcomas are more likely to come back than grade 1 tumors, and those that have spread beyond the uterus are more likely to return than those isolated to the uterus. Even so, women who have had leiomyosarcomas run the risk of having it return despite the stage and despite treatment after surgery. An often quoted risk is 50:50 with or without chemotherapy or radiation. Given this, a frank discussion with your doctor is very important when you are considering further treatment beyond surgery.
If your tumor recurs, then your doctor may recommend a repeat surgery to remove it. This is more likely if you have only one tumor seen or if you have recurred after a long time. If, after radiation or chemotherapy, the tumor grows quickly back, however, it is not likely that surgery will provide you any benefit. In either case, further treatment beyond surgery will be recommended. Standard drugs used for sarcomas include doxorubicin or docetaxel and gemcitabine (for leiomyosarcomas), or carboplatin and paclitaxel (for carcinosarcomas). Endometrial stromal sarcomas are treated with doxorubicin-based therapies.